You may be years out from your breast augmentation and suddenly asking questions you didn't expect to revisit. Do these implants still fit my body, my health priorities, and the way I want to look now? If you've been going back and forth between keeping them, removing them, or replacing volume in a more natural way, that uncertainty is normal.
Patients rarely come in with just one concern. Some are dealing with firmness, distortion, or rupture. Others feel done with implants and want relief, a softer silhouette, or a plan that doesn't trade one problem for another. Breast implant removal and reconstruction should never be approached as a one-size-fits-all procedure. It's a decision process.
Table of Contents
- The Explant Journey A Guide for Patients
- Why Women Choose Breast Implant Removal
- Your Surgical Consultation with Dr Yovino
- Understanding Your Primary Surgical Options
- Natural Reconstruction with Fat Transfer
- Your Recovery and Long Term Results
- Navigating Costs and Your Next Steps
The Explant Journey A Guide for Patients
A common moment goes like this. You get dressed, catch your reflection, and realize the question isn't whether your implants still look good. The question is whether they still feel right for your life. That shift matters.

This isn't a fringe decision. According to the ISAPS Global Survey 2023, approximately 335,939 breast implant removal procedures were performed worldwide in 2023, representing a 4.7% increase from 2022 and a 46.3% rise from nearly a decade earlier. More women are reconsidering implants for reasons that range from medical to aesthetic to personal.
What this journey really involves
Explant surgery sounds simple when reduced to a phrase like “implant removal.” In practice, decisions involved are broader:
- Whether removal alone is enough
- Whether the capsule should be left alone, partially removed, or fully removed
- Whether the breast needs a lift for shape
- Whether you want to restore volume using your own tissue rather than another implant
- Whether you're a candidate for an awake procedure under local anesthesia
Those choices affect scars, recovery, shape, softness, and how satisfied you feel months later.
Practical rule: The right explant plan starts with your anatomy and goals, not with internet terminology.
What patients need most
Most patients don't need more noise. They need a framework. They need help separating real surgical indications from social media myths, understanding what their breasts are likely to look like afterward, and deciding whether reconstruction should mean a lift, fat transfer, or letting the body return to a natural state.
That's how I think about breast implant removal and reconstruction. Not as a single operation, but as a guided process with trade-offs at every step. Some patients want the smallest intervention possible. Others want a full reshaping strategy. Both can be reasonable.
A good plan leaves you informed, realistic, and in control.
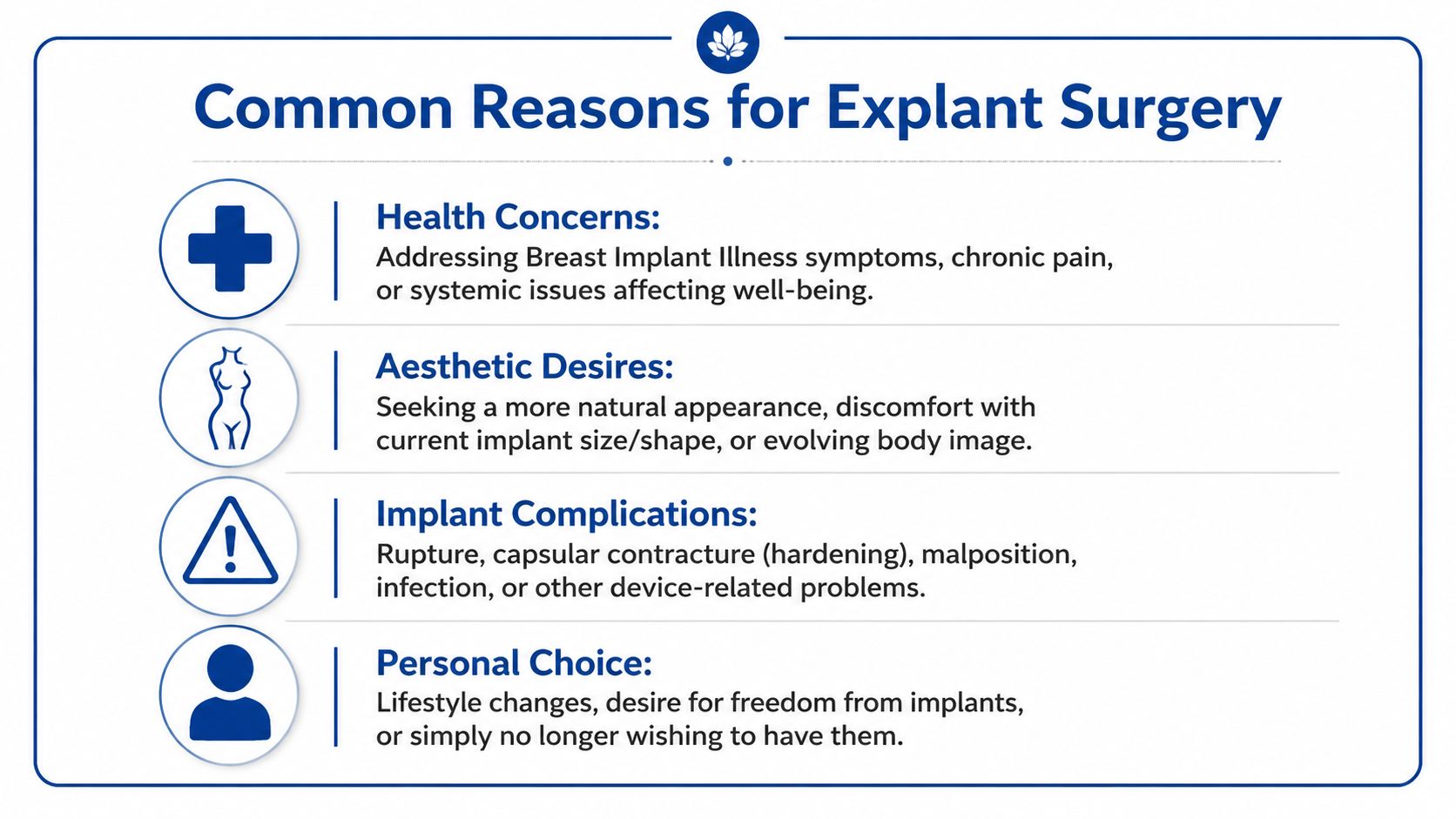
Why Women Choose Breast Implant Removal
No two patients arrive at this decision the same way. One patient is bothered by hardness and distortion. Another feels healthy but no longer wants implants in her body. Another has symptoms she believes may be related to her implants and wants a clear path forward. All of those reasons deserve a serious discussion.
Medical problems that push the decision
The clearest medical reasons for explant are usually structural. Capsular contracture is one of the most common. The scar capsule around the implant tightens, the breast can become firm or painful, and shape often changes. Sometimes the breast sits too high. Sometimes it looks round, distorted, or obviously artificial.
Rupture is another major reason. Saline rupture is usually obvious because the breast deflates. Silicone rupture can be far less obvious, which is why patients sometimes feel fine and still have a failed implant. Silent rupture can stay hidden until imaging or surgery reveals it.
Infection is less common, but it can force a more urgent conversation. The reported infection rate after surgery remains low at less than 1% in the clinical data on explantation and related outcomes in this multicenter longitudinal study of breast silicone explant. When infection progresses, implant removal may become necessary.
Systemic symptoms and Breast Implant Illness concerns
Some patients aren't driven by a visible implant problem. They come in because they don't feel like themselves. Fatigue, joint pain, brain fog, and other systemic complaints often come up in these consultations. Not every symptom has one cause, and a careful medical workup still matters, but these concerns shouldn't be dismissed.
Clinical research found that about 60% of symptomatic patients reported alleviation of complaints such as joint pain, fatigue, and cognitive issues following explantation in the same breast silicone explant study. That doesn't mean removal is a guaranteed cure for every patient. It does mean symptom improvement after explant is real enough to take seriously.
If your body has been telling you something feels wrong, the right next step isn't panic. It's a careful evaluation and a surgical plan based on facts.
Personal and aesthetic reasons are valid
A large share of explant decisions are personal. That matters because patients often apologize for it, as if wanting a different body now is somehow less legitimate than having a medical complication. It isn't.
Common non-medical reasons include:
- A more natural look: Many women want breasts that feel more in line with their current age, lifestyle, or self-image.
- Size fatigue: Implants that once felt proportionate can later feel too large, too noticeable, or physically cumbersome.
- Lifestyle changes: Exercise, motherhood, career changes, and shifting priorities all influence what feels comfortable.
- Freedom from maintenance: Some patients are tired of ongoing monitoring, uncertainty about rupture, or the prospect of future revision surgery.
In the explant literature, subjective reasons play a major role, especially earlier after augmentation. That matches what many surgeons see in practice. A patient doesn't need a dramatic medical event to decide she's done with implants.
The emotional layer
Explant is also an identity decision. Some patients feel relief the moment they schedule surgery. Others feel conflicted because the implants were tied to a different chapter of life. Both reactions can exist at once.
Here's what tends to work best emotionally. Make the decision from clarity, not fear. Understand what removal alone can achieve, where a lift helps, and when reconstruction with your own fat can improve shape without sending you back to another implant cycle.
Your Surgical Consultation with Dr Yovino
A strong consultation should feel less like a sales conversation and more like a planning session. In Beverly Hills, CA, the first visit is where I want to understand not just what you want removed, but what you want to wake up with afterward. That's the key question.
What gets evaluated
The exam is only one part of the consultation. I'm also looking at your surgical history, implant type if known, scar pattern, tissue thickness, skin elasticity, nipple position, and whether your concerns are primarily medical, aesthetic, or both. Those details shape whether you're a candidate for explant alone, explant with capsulectomy, a lift, or a natural volume-restoration strategy.
When patients have other ongoing health issues, preparation matters. If you're organizing medications, symptoms, and prior records before your visit, this guide on advice for managing chronic health conditions is a useful way to make the appointment more productive.
Questions worth bringing to the visit
Patients do better when they arrive ready to ask direct questions. These are the ones that usually change the quality of the discussion:
What is causing my concern?
Is the problem the implant, the capsule, stretched skin, breast position, or a combination?Do I need a capsulectomy, or is that being assumed?
Capsule treatment should be based on findings, not driven by fear-based language.What will my breasts likely look like if I remove the implants and do nothing else?
This is one of the most important questions in breast implant removal and reconstruction.Would a lift improve shape enough that I don't need added volume?
Sometimes reshaping matters more than size.Am I a candidate for an awake approach under local anesthesia?
Straightforward cases may allow for a modern office-based plan rather than general anesthesia.
What I want patients to leave with
By the end of the consultation, you should understand your options in plain language. You should know what's medically indicated, what's optional, and where the trade-offs are. You should also know if your goals are realistic.
What matters most: If a surgeon can't explain why a specific step is necessary for your anatomy, keep asking.
Some patients come in convinced they need an aggressive operation because of what they've read online. Others assume removal is simple and are surprised to learn a lift may be the difference between feeling empty and feeling balanced. The consultation is where those assumptions get corrected.
That clarity is what allows the next step to be confident rather than rushed.
Understanding Your Primary Surgical Options
Once the decision to remove implants is made, the next question is what combination of procedures will give you the most stable, honest result. Here, breast implant removal and reconstruction becomes strategic. The surgery isn't just about taking something out. It's about choosing what to preserve, what to reshape, and what to leave alone.
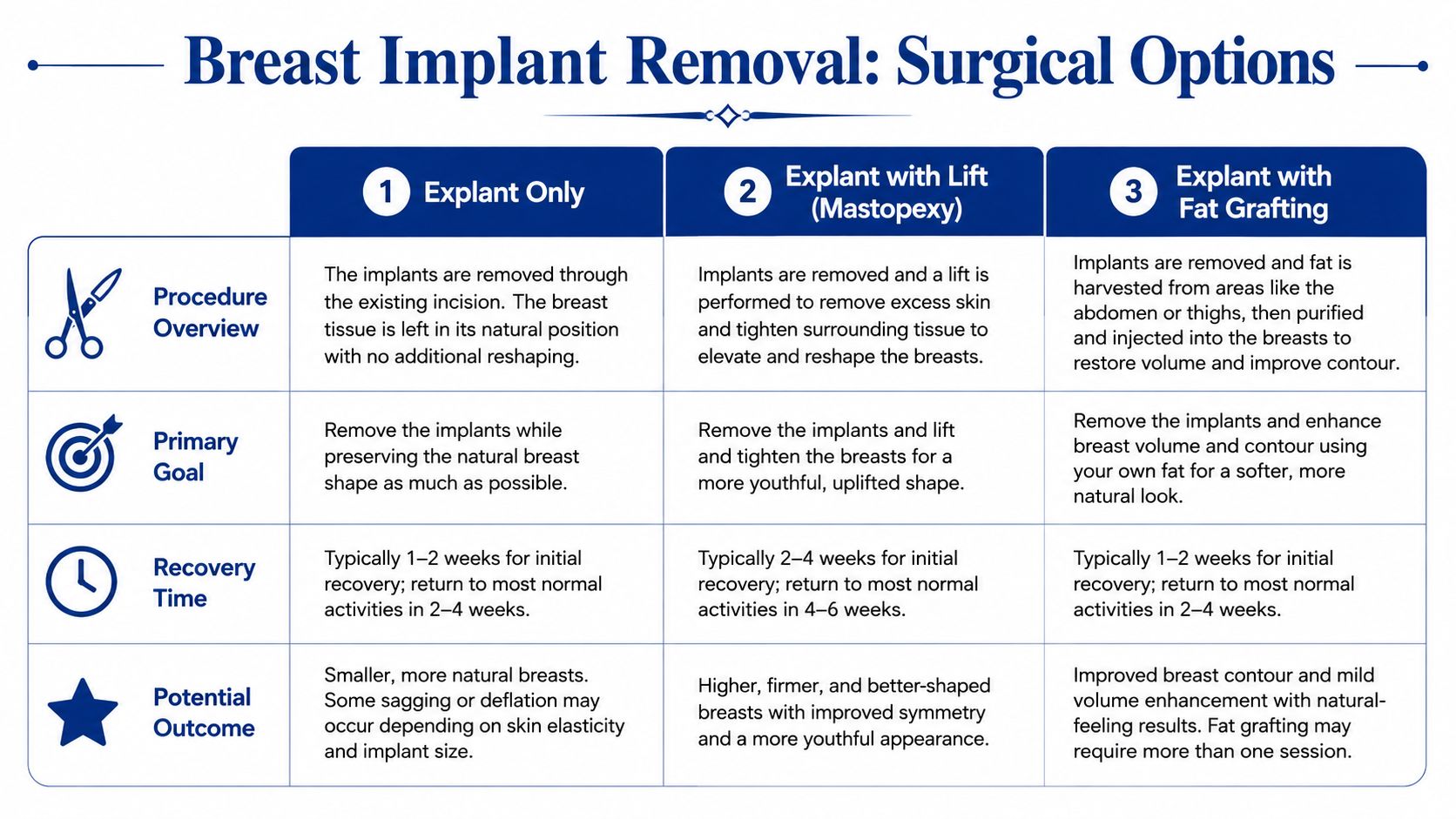
Explant only
This is the most limited option. The implant is removed, and the goal is to let the breast settle on its own without additional reshaping. It tends to suit patients with smaller implants, relatively strong skin recoil, and enough natural breast tissue to avoid a hollow look after removal.
The advantage is simplicity. Surgery is less extensive, recovery is usually more straightforward, and scars may be limited to prior incision sites. The downside is contour unpredictability. If the skin has been stretched or the nipple sits low, removal alone can leave the breast looking deflated.
Explant with capsulectomy
A capsulectomy addresses the scar tissue capsule surrounding the implant. Sometimes this is clearly indicated, such as when the capsule is thick, calcified, distorted, involved with rupture management, or otherwise abnormal. In other situations, only limited capsule treatment is needed.
This is where nuance matters. Patients often arrive believing the capsule always has to come out. That isn't supported by evidence in every scenario.
According to this review on capsulectomy and systemic benefit, capsule removal has never been proven to provide systemic benefit or reduce subsequent BIA-ALCL risk, with recurrence rates for contracture reaching up to 53% despite the procedure. That doesn't mean capsulectomy is never useful. It means it should be done for a specific reason.
The best capsule operation is the one that addresses the actual problem with the least unnecessary tissue trauma.
Explant with a breast lift
For many patients, shape is the primary issue after implant removal. The implant may have created upper fullness for years, while the skin and breast tissue gradually stretched. Once the implant is gone, the breast can sit lower and look flatter than expected.
A mastopexy, or breast lift, repositions and reshapes the breast. This doesn't replace implant volume, but it often improves contour dramatically by tightening the envelope and moving the nipple to a better position. For the right candidate, that's the difference between “empty” and “elegant.”
In select cases, an awake approach under local anesthesia can be part of that plan. That includes the kind of office-based breast reshaping used in an Awake Breast Lift, which may appeal to patients who want to avoid general anesthesia when their anatomy and procedure scope allow it.
The truth about en bloc removal
“En bloc” has become one of the most overused terms in explant discussions. Patients often hear it presented as the safest or most complete operation by default. That's not how surgical judgment works.
An intact en bloc removal means removing the implant and capsule together as a single unit. In standard cosmetic explant cases, that's often unnecessary and may require more dissection than the patient requires. A safer plan is frequently an individualized removal with capsule management based on findings rather than internet language.
Here's a practical comparison:
| Option | Main goal | Best fit | Main limitation |
|---|---|---|---|
| Explant only | Remove implant with minimal added surgery | Good skin elasticity, modest implant effect on tissues | Less control over final breast shape |
| Explant with capsulectomy | Remove implant and address problematic capsule | Contracture, rupture management, abnormal capsule findings | More surgical dissection |
| Explant with lift | Improve breast position and contour after removal | Ptosis, stretched skin, low nipple position | Adds scars and reshaping recovery |
Patients who want a broader overview of breast reshaping choices often benefit from reading more about what to know about breast reconstruction.
The right operation is usually not the most aggressive one. It's the one that solves the problem you have.
Natural Reconstruction with Fat Transfer
Not every patient who removes implants wants to stay exactly as she is after explant. Some want shape restored. Some want a softer upper pole. Some want modest volume, but have no interest in another device. That's where autologous reconstruction becomes useful.
How fat transfer fits into reconstruction
With fat transfer, fat is harvested from another area of your body through liposuction, then purified and placed into the breast to improve contour and add volume using your own tissue. The feel is natural because it is your tissue. The trade-off is that the result is more subtle than an implant and depends on how much fat survives after transfer.
For patients who want breast implant removal and reconstruction without going back to implants, this can be a very reasonable path. According to Cleveland Clinic's overview of breast implant removal, autologous fat transfer offers a viable alternative, with studies showing 30–50% volume retention after 12 months, though multiple sessions may be needed for optimal contour in techniques such as breast fat transfer result expectations.
That retention range is exactly why expectation-setting matters. Fat transfer is excellent for refinement and moderate restoration. It is not a shortcut to implant-sized projection in a single sitting.
Who tends to benefit most
Fat transfer tends to work well for patients who:
- Want a natural material only: No implant replacement, no foreign device.
- Have contour concerns more than size concerns: They want softness, transition, and balance rather than dramatic augmentation.
- Have donor fat available: The procedure depends on having usable fat to harvest.
- Accept staging when needed: More than one round may be appropriate for the best shape.
Some practices describe this style of reconstruction as a Raise Your Cup approach, meaning the focus is on natural shaping and selective volume restoration rather than trying to mimic the look of a large implant.
What works and what doesn't
What works is precision. Small-volume placement in the right tissue planes can smooth hollows, support cleavage shape, and reduce the deflated look that sometimes follows explant. What doesn't work is overselling fat transfer as if it can do everything an implant once did.
Fat grafting is strongest when it's used to improve contour, softness, and proportion. It's weakest when patients expect it to behave like an implant.
Some patients do better with a lift alone. Others need a lift plus fat transfer. A smaller group is satisfied with explant only. The reconstruction plan should follow the breast, not a trend.
One factual option among these approaches is that Ideal Face & Body offers fat transfer to the breasts as part of its surgical menu for patients who want autologous volume restoration after explant.
Your Recovery and Long Term Results
Recovery after explant surgery is usually less stressful when patients know what will change slowly and what should improve quickly. The early phase is about healing. The later phase is about settling, skin recoil, and adjusting to a new breast shape.
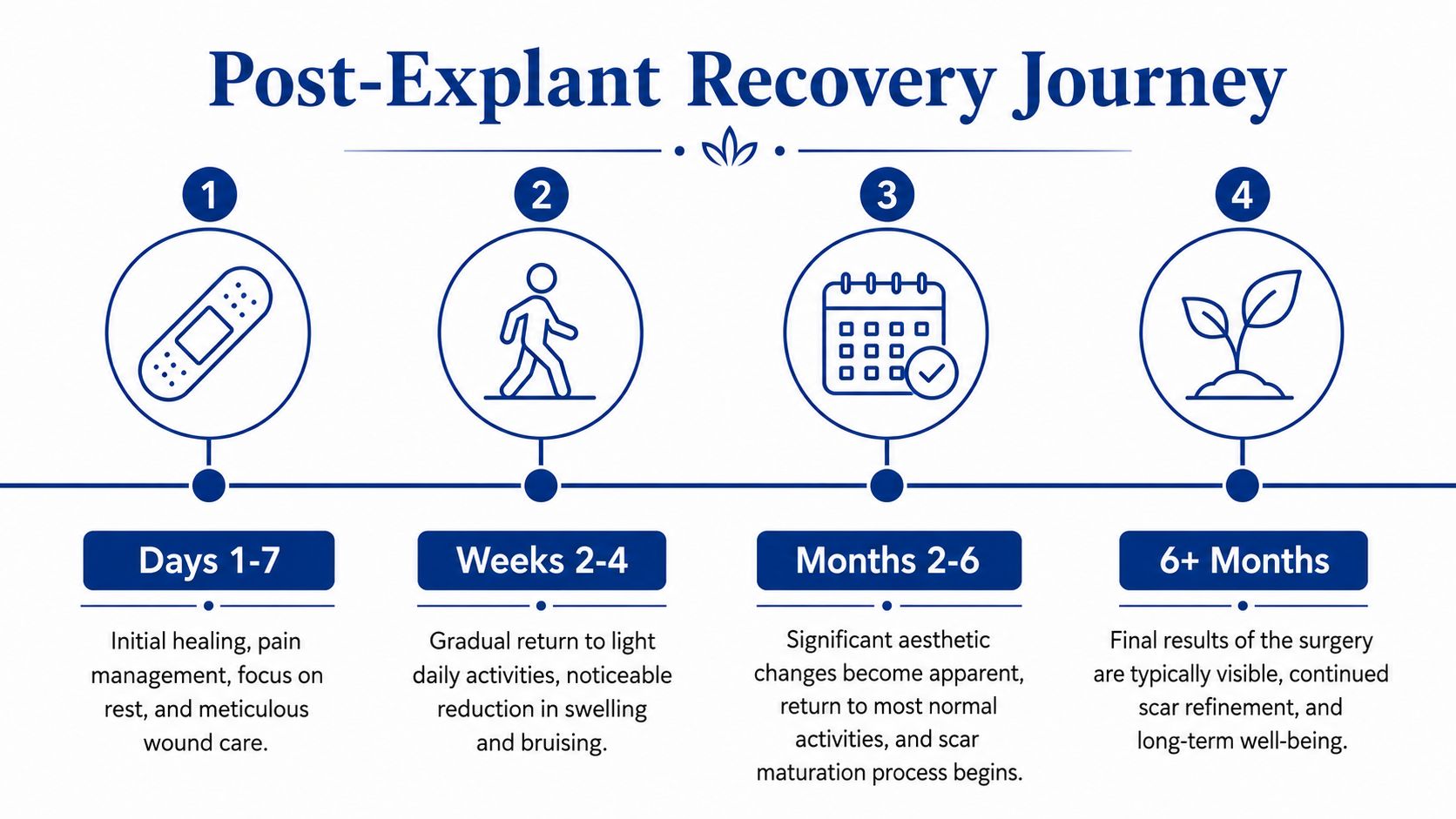
The first week
The first several days are usually defined by soreness, swelling, tightness, and fatigue. If you've also had a lift or capsulectomy, that recovery tends to feel more involved than explant alone. Support garments, wound care, and avoiding unnecessary upper-body strain matter early on.
An awake procedure under local anesthesia can change the feel of the immediate postoperative period for some patients. Avoiding general anesthesia may mean less of the fogginess and nausea that some patients dislike, although the breast tissues still need time to heal.
The next phase of healing
During the next few weeks, most patients gradually resume normal daily activity, then rebuild toward exercise and full routine. Based on the surgical review of explant recovery, full activity resumption typically requires 4–6 weeks, with final breast shape stabilizing over 3–6 months according to this clinical review on breast implant removal recovery.
That timeline matters because many patients judge the result too early. At first, the breast may look high, flat, wrinkled, swollen, or uneven. That doesn't mean something is wrong. It means tissues are still reorganizing.
A few practical guidelines help:
- Protect the repair: Don't test incisions, lifting restrictions, or range of motion before you're cleared.
- Expect shape changes: The appearance in week one is not the appearance at month three.
- Support the chest appropriately: Follow garment instructions closely, especially after a lift or fat grafting.
- Watch your emotions: It's common to feel relief and vulnerability at the same time.
When results start to look like you
The longer view is where most patients settle emotionally. As swelling fades and the skin retracts, the breast starts to look less like a recent surgical site and more like part of your body again. If reconstruction included fat transfer, volume also becomes more evident with time.
Patients recovering from more extensive breast surgery sometimes benefit from physical therapy principles that overlap with post-mastectomy rehabilitation, especially when chest tightness, posture, or guarded movement becomes part of recovery.
Healing goes better when you stop asking, “Do I look finished yet?” and start asking, “Am I progressing the way this operation usually progresses?”
Long-term success is usually less about perfection and more about alignment. Your breasts feel more natural, your symptoms or implant concerns are addressed, and the result fits the person you are now.
Navigating Costs and Your Next Steps
Patients often begin by asking what explant surgery costs. The honest answer is that costs vary because the procedure can range from simple implant removal to a more involved operation that includes capsule work, lifting, or natural reconstruction. The better question is what problem the surgery is solving, and what steps are needed to solve it safely.
Why insurance becomes the real obstacle
For many patients, the harder issue isn't the surgical fee. It's coverage. A major gap in public information is that health plans often deny explant claims by labeling them not medically necessary, even when the patient has significant symptoms or device-related problems. That problem is discussed directly in this guide to insurance coverage challenges for breast explant surgery.
That means patients need to think like advocates, not just like surgery shoppers.
Here are the practical moves that help:
- Gather documentation early: Operative reports, implant records, imaging, symptom history, and photographs can all matter.
- Ask for a focused medical necessity letter: It should explain your diagnosis, your symptoms or complications, and why surgery is being recommended.
- Read denial letters closely: Appeal deadlines can be short, and missing one can shut down options.
- Escalate when appropriate: Internal appeals are not always the end of the process.
What to do before surgery is scheduled
Before you commit to a date, make sure you understand whether you're paying privately, pursuing reimbursement, or trying for preauthorization. If you're looking for a general overview of factors that affect breast implant removal cost considerations, use it as a planning tool rather than a promise of what your case will require.
The bigger point is this. Don't let vague online language make the decision for you. Breast implant removal and reconstruction works best when the surgical plan matches your anatomy, your symptoms, and your priorities. Some patients need the simplest path. Others need reshaping. Others want a completely implant-free reconstruction using their own tissue.
The next step should be personal, not generic. If you're considering explant surgery in Beverly Hills, CA, a consultation with Dr. Justin Yovino can clarify what's necessary, what's optional, and whether an awake approach under local anesthesia makes sense for your case.
If you're ready to discuss breast implant removal and reconstruction with an individualized surgical plan, schedule a consultation with Ideal Face & Body. The goal is simple. Understand your options clearly, choose the approach that fits your body now, and move forward with confidence.